The multidisciplinary nature of Palliative and Hospice Care makes health care integration and local government support an important facet in improving the health of the people.
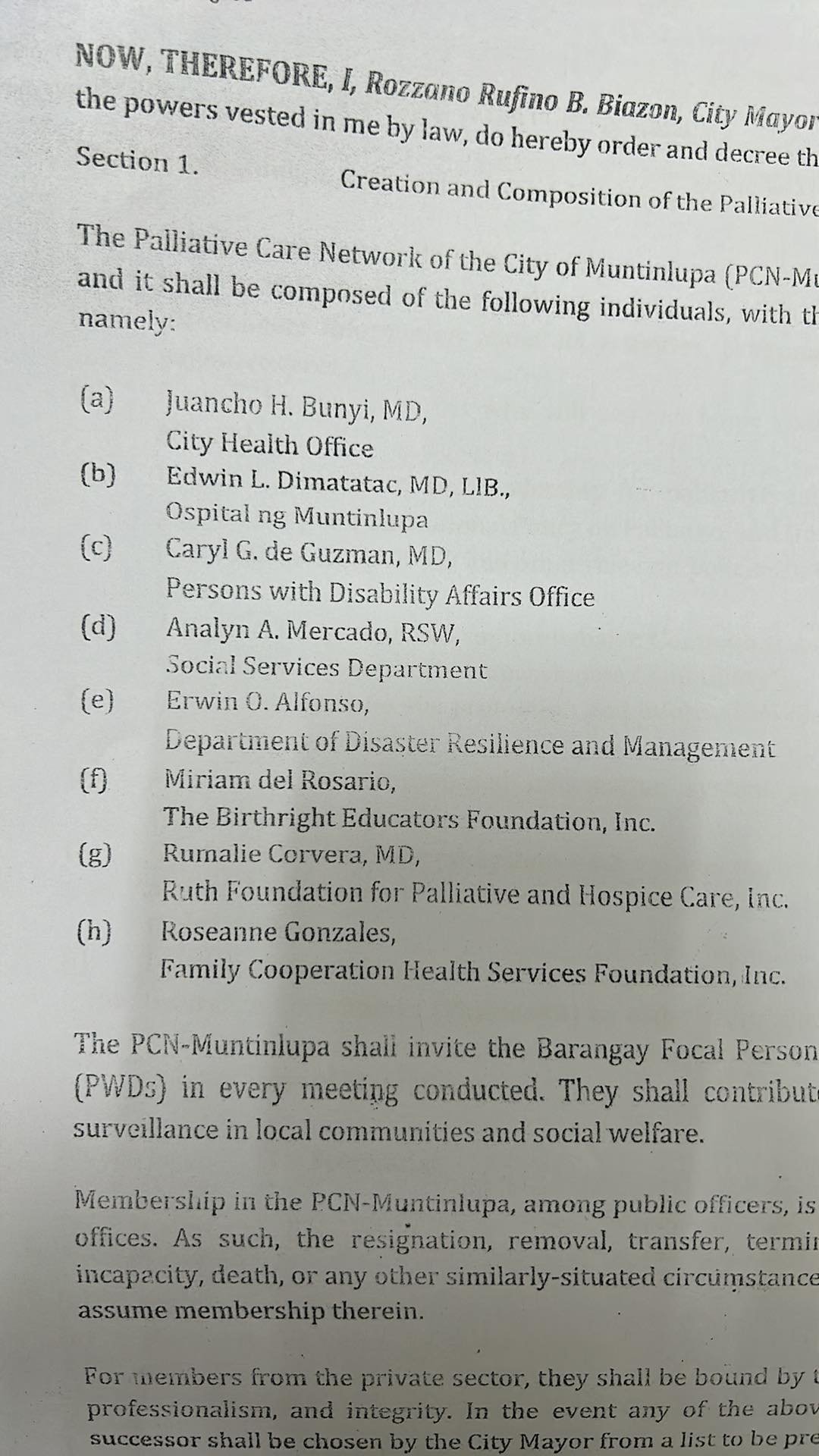
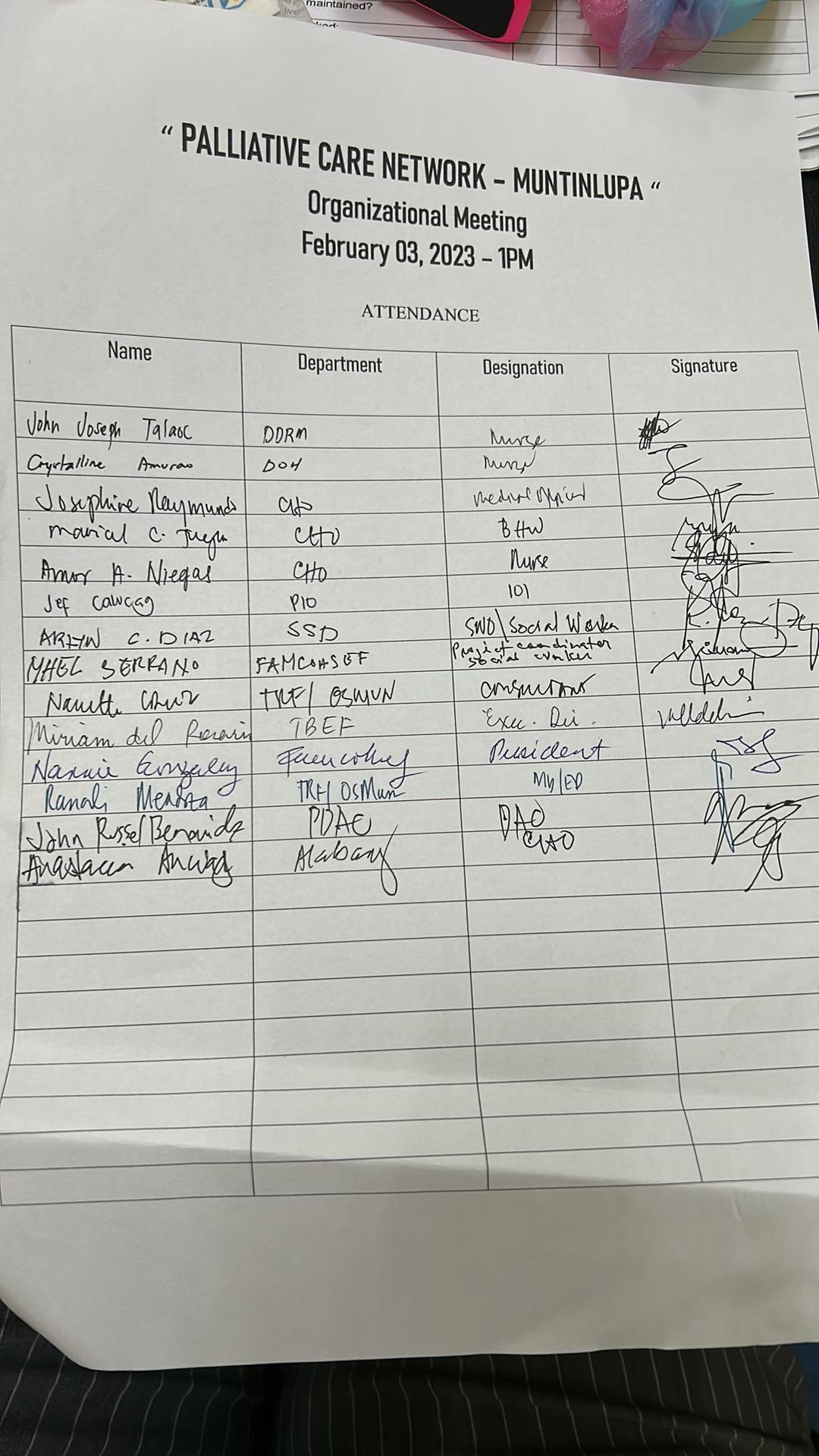
With the aim of providing health programs on primary health care, the City of Muntinlupa, in partnership with The Ruth Foundation for Hospice and Palliative Care (TRF), has created the Palliative Care Network (PCN). As approved by Muntinlupa City Mayor Rozzano Rufino “Ruffy” Biazon, PCN-Muntinlupa will be headed by its Chairperson, Dr. Juancho Bunyi (City Health Officer) with the participation of TRF CEO Dr. Rumalie Corvera, as one of its members.
PCN Muntinlupa will act as a sounding board for the provision of palliative care services in the city. Activities, programs, and training related to palliative care are expected to be put into place. It is also imperative that patient visits be conducted at home for those without the capability to travel to healthcare facilities.
To build a compassionate community rooted in scientific processes, PCN will also push for more evidence-based research on hospice and palliative care that will be published in peer-reviewed journals. The referral system is also going to be streamlined to create a more viable network for care provision and to lessen the stress of caregivers and families when trying to access care for their relatives with chronic illnesses. This will also be lined up with the comprehensive benefits package for Palliative Care in the Philippine Health Insurance Corporation.
The outcomes that can be expected from this network are immeasurable. It may not produce income, but it will create a more productive workforce that can focus on its economic needs instead of worrying about where to bring a relative who needs palliative care. A compassionate community encourages more empathy among its constituents, rekindling the “bayanihan” spirit of the Filipino where neighbors and friends help out in whatever capacity when someone is in need. Government officials would find more purpose in their activities, seeing that they make a difference in the lives of their constituents through hospice care. Businesses would create more socially relevant projects for palliative care and contribute their resources to generate goodwill. Religious leaders would find in hospice and palliative care a way to live out their teachings and provide counselling and support for those in distress.
In due time, PCN hopes that it can create a template that can be duplicated in other cities and municipalities. The Universal Health Care Law aims to provide Filipinos access to quality and cost-effective care. With proper planning, resource allocation, sound leadership, and determination to succeed, even those without the means to afford medical services can be given a life filled with dignity and hope. Local governments would also be able to instill a culture that is rooted on healthy lifestyles, disease prevention, and scientific management of disease and illness.
We would like to congratulate the City of Muntinlupa and The Ruth Foundation for its participation in this network. It is part of every individual’s vision to live a life that cultivates care and compassion. In the end, it is what makes us human. No amount of success and wealth can ever compensate for neglect at home and in the community we live in. Every man or woman is meant to look after each other in times of need.